
OB/GYN as the Front Door to Mental Health Care: New Evidence on Treating Perinatal Depression and Anxiety
Mental health conditions are a leading cause of pregnancy-related mortality in the United States, accounting for a significant portion of preventable maternal deaths. At the same time, most pregnant and postpartum individuals with symptoms of depression or anxiety do not receive treatment—even when those symptoms are identified in clinical care.
OB/GYN clinicians are often the most consistent point of contact during pregnancy and the postpartum period, placing them in a critical position to identify and respond to perinatal mental health needs. Screening for depression and anxiety is becoming more common. Access to timely, appropriate care has not kept pace.
A recent publication in the Maternal and Child Health Journal evaluates FamilyWell’s perinatal collaborative care model embedded within an OB/GYN practice. The study examines outcomes among pregnant and postpartum patients who screened positive for depression or anxiety and were referred into a structured behavioral health program delivered through a multidisciplinary care team.
The findings reflect care delivered in a real-world clinical setting, not a controlled research environment. To our knowledge, this is one of the first evaluations of a tech-enabled, coach-driven perinatal collaborative care model implemented in routine OB/GYN practice.
Study Overview: Perinatal Mental Health Care Embedded in OB/GYN
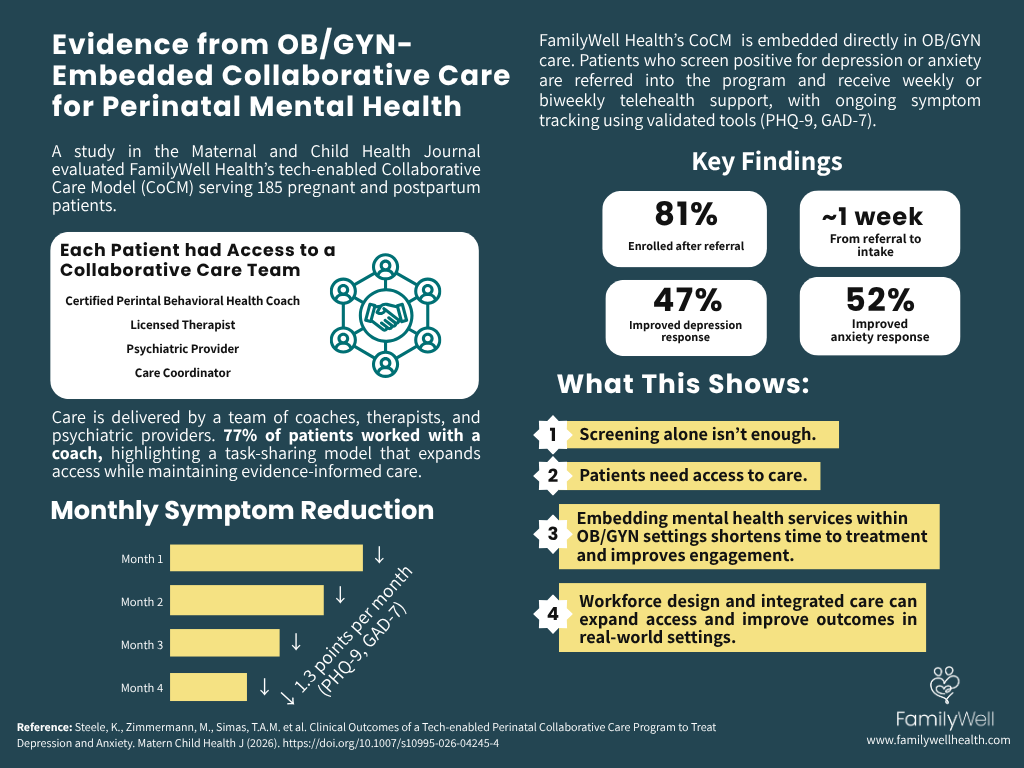
The study examined outcomes among 185 pregnant and postpartum patients receiving care through a collaborative care program embedded within an OB/GYN practice. Patients were identified through routine screening for depression and anxiety. Those who screened positive were referred into the program and offered structured behavioral health support.
Care was delivered through a multidisciplinary team that included certified perinatal behavioral health coaches, licensed therapists, and psychiatric providers. Patients participated in weekly or biweekly telehealth sessions, depending on clinical need and level of support.
Symptom severity was tracked over time using validated screening tools: the Patient Health Questionnaire-9 (PHQ-9) for depression and the Generalized Anxiety Disorder-7 (GAD-7) for anxiety. A 50% reduction in these scores is commonly used as a benchmark for clinically meaningful improvement.
The model also included clear pathways for escalation. Patients requiring higher levels of care were referred to licensed clinicians or psychiatric providers for additional support, ensuring that care was responsive to changes in symptom severity over time.
Key Findings
The study evaluated access, engagement, and clinical outcomes among patients receiving perinatal mental health care within an OB/GYN setting. Across these domains, the results show consistent patterns in both participation and symptom improvement over time.
Access and Engagement
A high proportion of patients who were referred into the program engaged in care. Eighty-one percent of referred patients enrolled, and 73% completed an initial intake appointment. The average time from referral to intake was approximately one week.
These timelines suggest that patients were able to move from identification to care quickly, with limited delays between referral and initial support.
Symptom Improvement Over Time
Among patients with moderate or higher symptom severity, both depression and anxiety scores decreased by an average of 1.3 points per month, as measured by PHQ-9 and GAD-7.
This pattern reflects steady symptom improvement over time, with patients showing consistent progress throughout the course of care.
Treatment Response
Nearly half of patients experienced a clinically meaningful reduction in symptoms. Forty-seven percent met criteria for depression response, and 52% for anxiety response.
These rates indicate that a substantial portion of patients experienced meaningful improvement during care.
Symptom Remission
A smaller but significant group of patients reached remission, with approximately 30% achieving low or minimal symptom levels. The average time to remission was between three and three and a half months.
These findings show that, for some patients, symptoms can resolve within a relatively short period when care is accessible and sustained.
Interpreting the Results
These findings provide a clear view into where perinatal mental health care continues to break down—and where it can improve.
Screening for depression and anxiety is becoming more common in OB/GYN settings. Identification alone does not ensure that patients receive care. In many systems, the gap emerges between screening and treatment, where referrals are made but not completed. The engagement rates observed in this study suggest that when care is accessible and closely connected to the clinical setting, more patients follow through.
The location of care also plays a role. Delivering behavioral health services within the OB/GYN setting allows patients to access support through an environment they already trust and engage with regularly. This continuity appears to support higher levels of participation compared to models that rely on external referrals.
Timing is another important factor. In this program, the average time from referral to intake was approximately one week. Shorter delays between identification and initial support allow patients to begin care earlier, which can influence both engagement and outcomes over time.
Together, these findings point to a consistent pattern: when access is immediate, care is integrated, and entry points are clear, more patients engage in treatment and remain connected to support.
The Role of Collaborative Care
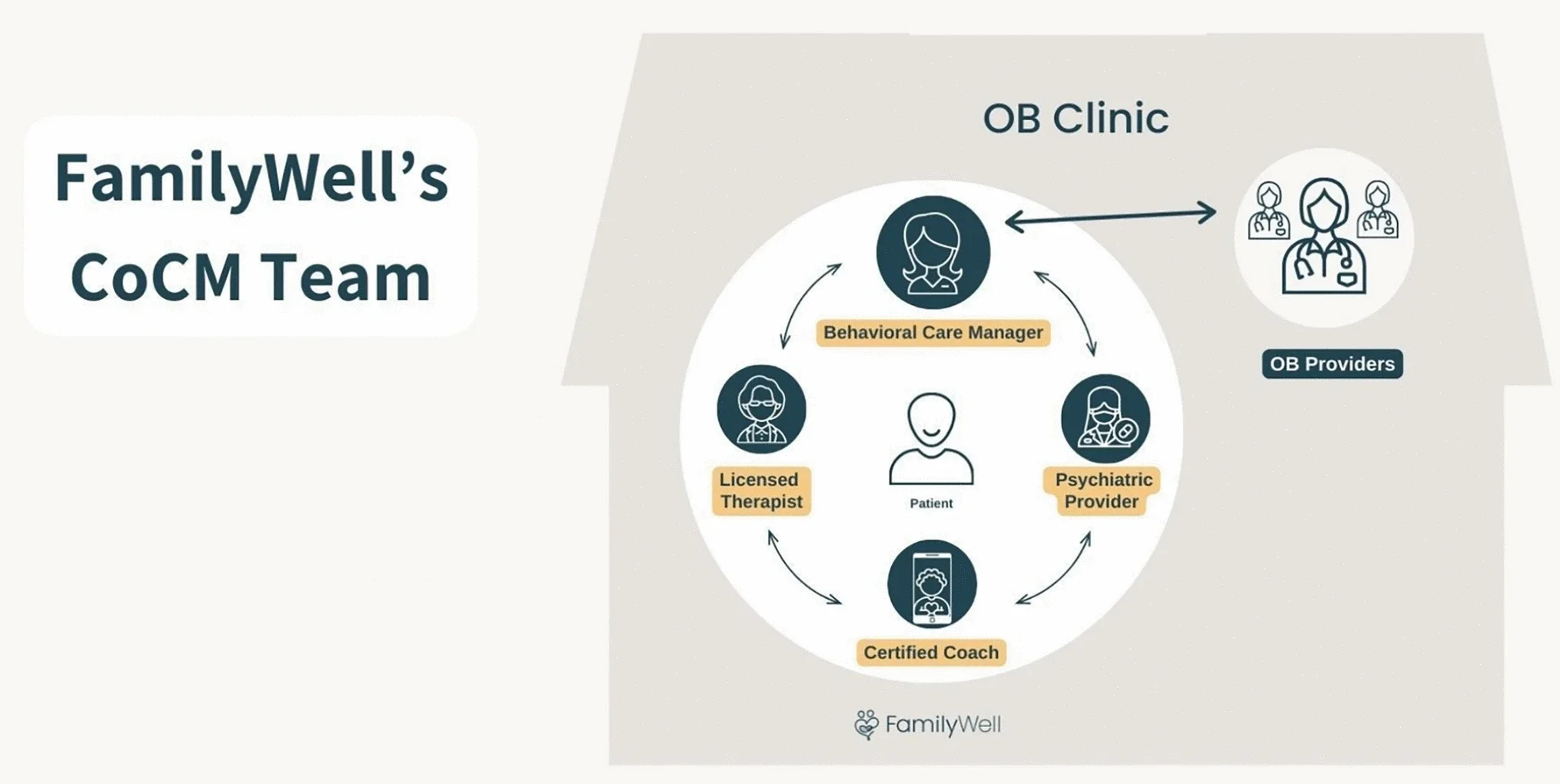
The program evaluated in this study is grounded in the Collaborative Care Model (CoCM), a team-based approach to behavioral health that has been widely studied across primary care and other medical settings. In this model, care is delivered by a multidisciplinary team that typically includes behavioral health providers, psychiatric consultants, and care coordinators working in close communication with the medical team.
Several core components define this approach. Care is measurement-based, meaning patient symptoms are tracked over time using validated tools such as the PHQ-9 and GAD-7. Treatment decisions are informed by these data, allowing the care team to adjust support based on patient progress. Regular case review is another key element, where complex cases are discussed among team members to guide clinical decision-making and ensure appropriate levels of care.
This structure allows for ongoing monitoring, coordination, and adjustment, rather than one-time referral or isolated treatment. The findings from this study reflect how this model performs when applied specifically within a perinatal OB/GYN setting, where patients are already engaged in regular medical care and where opportunities for early identification and intervention are more frequent.
Expanding the Perinatal Mental Health Workforce
A central component of this model is the integration of certified perinatal behavioral health coaches into the care team. In this study, 77% of patients received support from a coach as part of their care. Coaches provided structured, skills-based support, working alongside therapists and psychiatric providers within a coordinated system.
This approach reflects an intentional focus on workforce development. When asked about the origins of the model, FamilyWell CEO and founder Jessica Gaulton, MD, MPH emphasized the role of coaching in expanding access to care. As she explains, “I realized early on that coaching was the missing ingredient to meet patients where they are… we actually built the coaching program first, then added therapy and psychiatry.” She also notes that “coaches deliver over 75% of the care at FamilyWell,” which made specialized training essential to ensure quality and consistency across the model.
By embedding trained coaches into a multidisciplinary care team, this structure increases overall capacity and allows more patients to receive timely support. It also enables care to be delivered in a way that is responsive to varying levels of need, with clear pathways to escalate to clinical providers when appropriate.
Program Design and Delivery
The structure of the program supports both access and continuity of care. Services were delivered through a combination of telehealth sessions and SMS-based communication, allowing patients to engage with care in a way that fits into the realities of pregnancy and early parenthood. This approach reduces common barriers such as transportation, scheduling constraints, and childcare.
The program was also integrated directly into OB/GYN workflows. Patients were identified through routine screening and referred within the same clinical environment, creating a more seamless transition into behavioral health support. This integration supports coordination between medical and behavioral health providers and keeps care connected to the patient’s broader clinical experience.
Care delivery was supported by Collaborative Care Model (CoCM) billing codes, which allow for reimbursement of team-based, measurement-driven behavioral health services. This structure enables ongoing care rather than one-time interventions.
Symptom monitoring was conducted throughout treatment using validated tools, allowing the care team to track progress and adjust support as needed. Together, these components support consistent care delivery, ongoing monitoring, and the ability to scale the model across clinical settings.
Study Considerations
This study used a retrospective cohort design and did not include a control group, which limits causal conclusions. It was conducted within a single OB/GYN practice and included English-speaking patients with access to digital tools for telehealth and SMS-based care.
These factors may limit generalizability. Further research across diverse populations and settings is needed.
Implications for Perinatal Care
Screening alone does not improve outcomes without access to treatment. Patients need timely, structured support after symptoms are identified.
OB/GYN settings provide a practical point of integration for behavioral health care, given their consistent contact with patients during pregnancy and postpartum.
Workforce capacity remains a constraint. Expanding access will require models that extend beyond licensed providers and make use of task-sharing approaches. Roles such as Perinatal Behavioral Health Coaches allow for delivery of structured, skills-based support, while enabling clinical providers to focus on higher-acuity care. This distribution of responsibilities can increase reach without compromising care quality.
Final Thoughts
Patients in this model were able to access care quickly, with minimal delays between screening and initial support. Over time, symptoms of depression and anxiety improved, with a meaningful proportion of patients experiencing response or remission. These outcomes were observed in a real-world OB/GYN setting, reflecting how care is delivered in routine practice.
As screening for perinatal mental health conditions continues to expand, care systems need to ensure that patients can access timely, integrated support within the settings where they already receive care.
Frequently Asked Questions
What is collaborative care in OB/GYN?
Collaborative care is a team-based model that integrates behavioral health services into medical settings such as OB/GYN practices. In this approach, patients receive support from a coordinated team that may include behavioral health coaches, therapists, psychiatric providers, and OB clinicians. Care is measurement-based, meaning symptoms are tracked over time using validated tools, and treatment is adjusted based on patient progress. This model allows patients to access mental health support within the same setting where they receive routine prenatal and postpartum care.
How is perinatal depression treated?
Perinatal depression is typically treated through a combination of approaches depending on symptom severity and patient needs. These may include psychotherapy, medication, behavioral strategies, and social support. In collaborative care models, treatment is coordinated across providers to ensure continuity and appropriate levels of support. Patients with mild to moderate symptoms may benefit from structured behavioral support and coaching, while those with more severe symptoms may require clinical care from licensed therapists or psychiatric providers.
What does a perinatal behavioral health coach do?
A Perinatal Behavioral Health Coach (PBHC) provides skills-based emotional support during pregnancy and the postpartum period. Coaches help patients manage symptoms such as anxiety, stress, and intrusive thoughts by teaching practical strategies, supporting behavior change, and offering ongoing guidance. They are part of a broader care team and work alongside therapists and psychiatric providers, helping extend access to care and ensuring patients receive timely support.
Why is early mental and behavioral health treatment important postpartum?
Early treatment is important because symptoms of depression and anxiety can affect both the parent and the developing infant if left unaddressed. Timely support can reduce symptom severity, improve functioning, and support bonding and caregiving. Early intervention also increases the likelihood of recovery and can prevent symptoms from worsening over time.
Read the full article at:
Steele, K., Zimmermann, M., Simas, T.A.M. et al. Clinical Outcomes of a Tech-enabled Perinatal Collaborative Care Program to Treat Depression and Anxiety. Matern Child Health J (2026). https://doi.org/10.1007/s10995-026-04245-4