
Understanding Perinatal Mood and Anxiety Disorders (PMADs): A Guide for Providers

Perinatal mood and anxiety disorders (PMADs) are very common, yet most providers do not know what to look for in patients or how to help if they suspect it’s more than just the Baby Blues.
“I think I’m just really tired… but something feels off.”
Perinatal providers hear versions of this often. A patient may describe feeling overwhelmed, unusually anxious, or like they are somehow “doing something wrong.” It may be normal new-parent exhaustion or worry —but sometimes, when providers pause and ask a few more questions, a different story emerges.
Pregnancy and the postpartum period involve profound biological, psychological, and social change, and, while these stages can be accompanied by plenty of joy and excitement, they are also one of the highest-risk periods for the onset or worsening of mental health conditions. Hormonal shifts, sleep disruption, identity changes, and the demands of caring for a newborn can all affect emotional well-being.
When symptoms persist or begin to interfere with daily functioning, they may fall under the umbrella of Perinatal Mood and Anxiety Disorders (PMADs)—a group of mental health conditions that can occur during pregnancy and throughout the first year postpartum. While postpartum depression is the most widely recognized, PMADs also include anxiety disorders, obsessive–compulsive symptoms, trauma-related responses, and, in rare cases, postpartum psychosis.
Recognizing these conditions early is key. When providers listen closely and ask the right questions, many PMADs can be identified sooner and treated effectively.
What Are Perinatal Mood and Anxiety Disorders (PMADs)?
Perinatal Mood and Anxiety Disorders (PMADs) is an umbrella term used to describe a group of mental health conditions that can occur during pregnancy and throughout the first year after childbirth. While the postpartum period is often associated with emotional adjustment, PMADs refer to clinically significant mood or anxiety symptoms that go beyond the typical stress or temporary mood fluctuations many new parents experience.
The perinatal period is marked by substantial biological, psychological, and social changes. Hormonal shifts, sleep disruption, identity transitions, physical recovery from childbirth, and evolving family dynamics can all affect mental health. For some individuals, these stressors contribute to the development or worsening of mental health conditions.
Understanding the range of PMAD presentations helps providers recognize symptoms earlier and connect patients with appropriate support.
How Common Are Perinatal Mood and Anxiety Disorders?
Perinatal Mood and Anxiety Disorders (PMADs) are among the most common complications of pregnancy and childbirth. Research consistently shows that approximately 1 in 5 women experience a mental health condition during pregnancy or within the first year postpartum. Despite their prevalence, many cases remain undetected and untreated, leaving parents without the support they need during a vulnerable period.
For some individuals, changes that affect their mental health are temporary and manageable. For others, they can interact with existing vulnerabilities or stressors and contribute to clinically significant symptoms. Recognizing how common PMADs are—and understanding the factors that contribute to them—can help providers normalize conversations about mental health and support earlier identification
Common Types of PMADs
Postpartum Depression
"I thought I’d feel more connected to the baby by now. Instead, I just feel numb… like I’m going through the motions."
Postpartum depression is the most commonly recognized perinatal mental health condition. It occurs in about 15% of postpartum women, and it involves persistent low mood beyond the “baby blues” and loss of interest or pleasure in activities that previously felt meaningful. While fatigue and emotional fluctuations can be normal after childbirth, postpartum depression is characterized by symptoms that persist and interfere with daily functioning.
Common symptoms may include:
Persistent sadness or low mood
Fatigue or low energy beyond typical sleep deprivation
Loss of interest in activities once enjoyed
Feelings of guilt, inadequacy, or failure as a parent
Some individuals may also experience irritability, difficulty concentrating, changes in appetite, or feelings of emotional numbness.
Postpartum Anxiety (PPA)
"Even when the baby is sleeping, I can’t relax. I feel like I have to stay on alert all the time."
Anxiety disorders are highly prevalent during the perinatal period and may occur independently or alongside depression. A cross-sectional study found that about 1 in 5 women experience postpartum anxiety (PPA). Postpartum anxiety often presents as persistent and intrusive worry that feels difficult to control.
Common symptoms may include:
Excessive worry about the baby’s health or safety
Racing or repetitive thoughts
Physical tension, restlessness, or difficulty relaxing
Difficulty sleeping even when the baby is resting
Many parents experiencing postpartum anxiety report feeling constantly “on edge” or unable to quiet their thoughts. If the onset of the anxious thoughts and feelings appear prior to giving birth, it is referred to as perinatal anxiety.
Postpartum Obsessive–Compulsive Disorder (OCD)
"I know it sounds irrational, but I keep thinking something bad will happen if I don’t check the baby again. I’ll go back into the room over and over just to make sure everything is okay."
Perinatal OCD involves intrusive, unwanted thoughts paired with repetitive behaviors or mental rituals intended to reduce distress. Intrusive thoughts may involve fears of accidental harm coming to the baby or distressing mental images that feel inconsistent with the parent’s values.
These thoughts are ego-dystonic, meaning they are experienced as disturbing, unwanted, and inconsistent with the individual’s intentions. Importantly, individuals with postpartum OCD are typically deeply distressed by these thoughts and take steps to avoid acting on them.
Recent studies conclude that OCD symptoms can develop in about 7.8% of pregnancies and prevalence increases to 16.9% across the postpartum period.
Symptoms may include:
Intrusive thoughts or images about harm coming to the baby
Compulsive checking behaviors
Repetitive cleaning or safety rituals
Mental reviewing or reassurance seeking
Because these thoughts can feel frightening or shameful, many parents hesitate to disclose them unless directly asked in a supportive environment.
Postpartum Post-Traumatic Stress Disorder (PTSD)
"Every time I think about the birth, my heart starts racing. I can’t stop replaying it in my head."
Some individuals experience symptoms of post-traumatic stress following childbirth, particularly if the birth involved perceived or actual threats to the parent or infant.
Common triggers include:
traumatic birth experiences
emergency interventions
feelings of loss of control during labor or delivery
Symptoms may include intrusive memories of the birth, avoidance of reminders, heightened anxiety, or difficulty processing the experience.
Studies have varied estimates of the prevalence of postpartum PTSD with the estimated prevalence ranging between 3.1% and 24.5% worldwide.
Postpartum Psychosis
"I’m not sleeping at all, and things just feel… strange. Sometimes I hear things or feel like something is wrong that I can’t explain."
Postpartum psychosis is a severe condition that occurs between 1 to 2 per 1000 women after delivery. While rare, it is a severe psychiatric condition that typically develops within the first few weeks after childbirth. It involves a loss of contact with reality and requires emergent psychiatric evaluation and treatment.
Symptoms may include:
confusion or disorientation
hallucinations or delusional beliefs
extreme mood swings
paranoia or unusual behavior
Reduced need for sleep
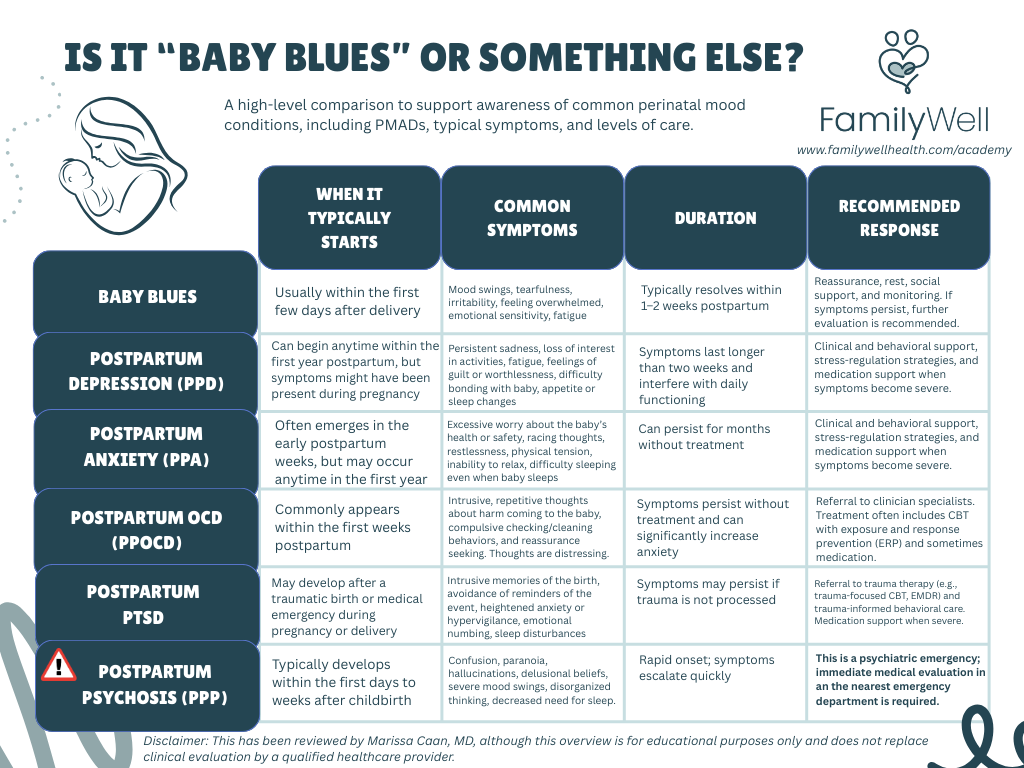
This medically-reviewed table provides an overview of common PMADs as compared to Baby Blues.
Postpartum psychosis is considered a psychiatric emergency as it could put the mother and her family at risk. Immediate medical attention is essential to ensure the safety of both the parent and infant..
Why PMADs Often Go Undetected
Despite how common Perinatal Mood and Anxiety Disorders are, many cases remain unrecognized and untreated. Multiple structural, cultural, and clinical factors contribute to this gap.
Stigma Around Maternal Mental Health
One major barrier is stigma surrounding mental health during pregnancy and postpartum. Many parents feel pressure to present the transition to parenthood as joyful and fulfilling, which can make it difficult to acknowledge distress. Feelings of shame, fear of judgment, or concerns about being perceived as an “unfit parent” may lead individuals to minimize symptoms or avoid discussing them altogether.
The Normalization of Postpartum Struggle
PMADs are also frequently overlooked because emotional struggles during the postpartum period are often normalized as part of new parenthood. Exhaustion, irritability, and emotional overwhelm are common experiences after childbirth, and patients themselves may assume what they are feeling is simply “part of the adjustment.” As a result, symptoms that might otherwise signal depression or anxiety may go unrecognized.
Limited Time in Postpartum Care
Structural constraints within healthcare systems can further limit detection. In many care models, postpartum care includes one routine visit around six weeks after delivery, and appointments are often brief. During these visits, providers must address multiple concerns—physical recovery, contraception, breastfeeding, and infant care—leaving limited time to explore emotional well-being in depth.
Low Screening Rates in Practice
Even when validated screening tools exist, they are not always consistently implemented. Analyses of National Committee for Quality Assurance (NCQA) data found that prenatal depression screening occurred in only about 13% of Medicaid patients and about 5% of commercially insured patients, with postpartum screening rates even lower. These gaps mean that many patients experiencing symptoms may never be formally assessed.
Workforce Gaps in Perinatal Mental Health
The shortage of providers trained in maternal mental health also contributes to under-detection and undertreatment. Many regions face long wait times for therapy and limited access to clinicians with specialized training in perinatal mental health (Byatt et al., 2019). When referral pathways are unclear or resources are scarce, screening may feel less actionable for providers.
Symptoms Are Often Described Indirectly
Finally, patients themselves often describe symptoms indirectly rather than naming depression or anxiety. Instead of saying they feel depressed, they may describe their experience in more general terms.
For example:
“I feel like I’m failing at this.”
“I’m exhausted all the time and can’t get it together.”
“I should be happier than I am.”
These types of statements can reflect underlying emotional distress but may be missed if providers are focused primarily on physical recovery or infant care. Recognizing these cues—and creating space for open conversation about mental health—can help providers identify PMADs earlier and connect patients with appropriate support.
How Providers Can Help Detect PMADs Early
Early detection is one of the most effective ways to reduce the impact of Perinatal Mood and Anxiety Disorders.
Because many patients may not spontaneously disclose mental health concerns, providers who work with pregnant and postpartum populations, including L&D nurses, OBs, doulas, therapists, perinatal behavioral health coaches, perinatal mental health coaches, and PMH-Cs, play a critical role in normalizing conversations about emotional well-being and implementing routine screening practices.
Routine Mental Health Screening
Clinical guidelines increasingly recommend universal mental health screening during pregnancy and the postpartum period. Validated screening tools can help identify symptoms early and create structured opportunities for patients to discuss how they are feeling.
Commonly used screening tools include:
Edinburgh Postnatal Depression Scale (EPDS) – a widely used screening tool designed specifically for perinatal depression and anxiety.
Patient Health Questionnaire-9 (PHQ-9) – a general depression screening tool commonly used in primary care settings.
Generalized Anxiety Disorder-7 (GAD-7) – a brief tool used to assess symptoms of anxiety.
Screening is most effective when it occurs at multiple points across the perinatal period, rather than as a single check-in. Opportunities may include:
Prenatal visits
Postpartum visits
Pediatric well-baby visits
Because pediatric providers often see families frequently in the first year of life, they can play an important role in identifying concerns that may otherwise go unnoticed.
Creating Safe Conversations Around Mental Health
Screening tools are helpful, but they work best when paired with supportive, nonjudgmental conversations. Many patients hesitate to disclose symptoms because they worry about being judged or misunderstood.
Simple language that normalizes the experience can help open the door. For example:
“Many new parents experience emotional changes during pregnancy and after birth. How have you been feeling emotionally lately?”
When providers routinely ask about mental health alongside physical recovery, it sends a clear message that emotional well-being is an expected and important part of care.
Building Referral Pathways and Support Networks
Not everyone working with perinatal families is a licensed mental health clinician. Doulas, lactation consultants, health coaches, childbirth educators, and community-based providers including Perinatal Behavioral Health Coaches often develop close relationships with parents and may be among the first to notice signs of distress.
For non-clinical providers, an important step is building a network of referral resources ahead of time. This might include identifying:
therapists who specialize in perinatal mental health
psychiatric providers experienced in treating PMADs
local support groups or community organizations
crisis and emergency resources
Having these connections in place makes it easier to guide patients toward appropriate care if concerns arise.
Recognizing Red Flags
While many patients experience mild to moderate emotional distress during pregnancy and the postpartum period, some symptoms indicate a need for urgent clinical evaluation. Providers who work with perinatal families should be familiar with these warning signs and know how to respond quickly.
Red flags that warrant immediate attention include:
Persistent low mood that does not improve or continues to worsen
Severe or escalating anxiety that interferes with daily functioning
Intrusive thoughts accompanied by a desire or intent to act on them
Inability to function, including difficulty caring for oneself or the infant
Thoughts of self-harm or suicidal ideation
Extreme sleep deprivation, especially when a parent cannot sleep even when the baby is resting
Hallucinations, including hearing or seeing things others do not perceive
Confusion, paranoia, or disorganized thinking
These symptoms may indicate a severe mood disorder or another psychiatric condition that requires immediate clinical care.
For providers who are not mental health clinicians—such as doulas, coaches, lactation consultants, or childbirth educators—the key role is recognition and rapid referral. When red flag symptoms appear, encouraging the patient and their family to seek immediate medical care may be life-saving.
Expanding Support Through Collaborative Care
Many clinics are also exploring ways to expand mental health support within perinatal care teams. In collaborative care models, behavioral health professionals, coaches, and medical providers work together to support patients across different levels of need.
For example, Perinatal Behavioral Health Coaches (PBHCs) may help patients implement behavioral strategies, monitor mood symptoms, and reinforce care plans while maintaining close communication with clinical providers. These types of integrated models can improve access to support while ensuring that patients who need therapy or psychiatric care are referred appropriately.
Some OB practices partner with organizations like FamilyWell to incorporate structured perinatal behavioral health coaching into their care models, helping patients receive ongoing support between clinical visits.
Supporting Patients With PMADs
For individuals experiencing mild to moderate symptoms, supportive interventions can often be very effective. Providers frequently meet patients who are trying their best to care for their baby while quietly struggling with worry, low mood, or exhaustion. In these cases, structured support and practical coping strategies can make a meaningful difference.
These may include:
Support groups that reduce isolation and normalize common challenges in early parenthood
Behavioral health coaching, which can help patients build routines, implement behavioral strategies, and monitor mood changes over time
Behavioral support techniques such as behavioral activation, stress regulation strategies, and sleep-supportive routines
Increased social support, including peer networks and community resources
Perinatal Behavioral Health Coaches (PBHCs), for example, often help patients implement practical strategies—such as increasing light exposure, establishing daily structure, and re-engaging with meaningful activities—that support mood stabilization and emotional well-being.
When symptoms become more severe, clinical treatment is typically necessary. Evidence-based care may include:
Psychotherapy, such as cognitive behavioral therapy (CBT), trauma therapy, or interpersonal therapy (IPT), among others
Medication, prescribed and monitored by a qualified medical provider
Specialized psychiatric care for complex or high-risk conditions
In these situations, behavioral support professionals, like perinatal behavioral health coaches, may still play a complementary role. While licensed clinicians manage diagnosis and treatment, behavioral health coaches can help patients apply therapeutic strategies in daily life, reinforce care plans, and monitor changes in symptoms between appointments.
Conclusion: Improving Maternal Mental Health Starts With Awareness
Perinatal Mood and Anxiety Disorders are common, yet they often go unrecognized. For many families, the difference between prolonged suffering and early recovery is simply whether symptoms are identified and addressed in time. Increasing awareness of PMADs among healthcare providers, community professionals, and families is a critical step in improving maternal mental health outcomes.
References
ACOG Committee Opinion No. 736: Optimizing Postpartum care. (2018). Obstetrics and Gynecology, 131(5), e140–e150. https://doi.org/10.1097/aog.0000000000002633
Alemu, S. S., Jarso, M. H., Gejo, N. G., Hebo, H. J., Bedecha, D. Y., Bekele, F., Gezimu, W., Demsash, A. W., Teferi, S. M., Kitil, G. W., Dube, G. N., Yimer, A. A., Kebede, B. N., Bekele, G. G., & Wedajo, L. F. (2024). Prevalence of postpartum post-traumatic stress disorder and associated factors among postnatal mothers in West Arsi zone, South West Ethiopia, 2024: a community-based cross-sectional study. Frontiers in Psychiatry, 15, 1470819. https://doi.org/10.3389/fpsyt.2024.1470819
Britt, R., & Britt, R. (2025, November 24). The latest HEDIS Maternal Mental health screening rates. Policy Center for Maternal Mental Health. https://policycentermmh.org/the-latest-hedis-maternal-mental-health-screening-rates/
Byatt, N., Levin, L. L., Ziedonis, D., Simas, T. a. M., & Allison, J. (2015). Enhancing participation in depression care in outpatient perinatal care settings. Obstetrics and Gynecology, 126(5), 1048–1058. https://doi.org/10.1097/aog.0000000000001067
Byatt, N., Xiao, R. S., Dinh, K. H., & Waring, M. E. (2015). Mental health care use in relation to depressive symptoms among pregnant women in the USA. Archives of Women S Mental Health, 19(1), 187–191. https://doi.org/10.1007/s00737-015-0524-1
Can we identify women at high risk for postpartum psychosis? (2009, August 3). MGH Center for Women’s Mental Health. https://womensmentalhealth.org/posts/can-we-identify-women-at-high-risk-for-postpartum-psychosis/
Hemstad, M. (2025, August 1). Maternal Mental health Conditions and Statistics: An overview — Maternal Mental Health Leadership Alliance: MMHLA. Maternal Mental Health Leadership Alliance: MMHLA. https://www.mmhla.org/articles/maternal-mental-health-conditions-and-statistics
High Prevalence of OCD in Pregnant and Postpartum Women. (2021, May 6). https://womensmentalhealth.org/posts/high-prevalence-of-ocd-in-pregnant-and-postpartum-women/
MGH Center for Women’s Mental Health. (n.d.). Psychiatric Disorders during Pregnancy: Weighing the risks and benefits of pharmacologic treatment during pregnancy. https://womensmentalhealth.org/specialty-clinics/psychiatric-disorders-during-pregnancy/
Postpartum Support International. (2026, February 3). Perinatal/Postpartum psychosis help | Postpartum Support International (PSI). Postpartum Support International (PSI). https://postpartum.net/get-help/postpartum-psychosis-help/
Qin, Z., Pan, Y., Yang, H., Luan, L., Zhang, X., & Zhu, C. (2025). Prevalence and risk factors of postpartum depression, anxiety, and comorbidity of both disorders: a cross-sectional study. BMC Pregnancy and Childbirth, 25(1), 1352. https://doi.org/10.1186/s12884-025-08512-0
Raza, S. K., & Raza, S. (2023, June 26). Postpartum psychosis. StatPearls - NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK544304/
Screening and diagnosis of mental health conditions during pregnancy and postpartum. (2023, June). ACOG. https://www.acog.org/clinical/clinical-guidance/clinical-practice-guideline/articles/2023/06/screening-and-diagnosis-of-mental-health-conditions-during-pregnancy-and-postpartum
What to Expect at a Postpartum Checkup—And Why the visit matters. (n.d.). ACOG. https://www.acog.org/womens-health/experts-and-stories/the-latest/what-to-expect-at-a-postpartum-checkup-and-why-the-visit-matters